
{kind=link}
When I come to the last post of a year, I sometimes like to look back at the year that has passed and then perhaps make some observations over what I think might happen in the year to come. For instance, last year at this time I declared 2023 to be the year that the evidence-based medicine model, specifically the dogmatic version that dismisses any evidence that doesn’t come from randomized controlled trials as being basically crap, had been weaponized against public health interventions ranging from masks to “lockdowns” to vaccines. Other examples include characterizing 2021 as the year that “everything [antivax and quackery] old is new again” and 2020 as the year of physicians behaving badly, because of a disturbing number of physicians who had up to that point been seemingly respectable taking a heel turn to COVID-19 minimization, attacks on public health, and even outright quackery. Unfortunately, all of those things that characterized those years continued in 2024—on steroids!—which led me to go back to what I said about one year that I left out above, specifically 2022. That was the year that a certain antivax activist characterized as the year of “gaslighting” COVID-19.
Why go back to that year? As I like to say, when it comes to conspiracy theorists and science deniers, every accusation is a confession. Since Donald Trump won the 2024 Presidential election and has nominated a rogues’ gallery of quacks, antivaxxers, and grifters for key federal health posts, all led by longtime antivax activist Robert F. Kennedy Jr., whom President-Elect Trump has nominated to be Secretary of Health and Human Services, I see gaslighting everywhere. Indeed, his allies and apologists are engaged in a propaganda program of deception, revisionist history, and outright misinformation to try to minimize or outright deny RFK Jr.’s antivax views, conspiracy theories, and the harm that he had already done to public health prior to 2024. In particular, lately I’ve been seeing RFK Jr. apologists try desperately to gaslight his personal role in stoking antivaccine beliefs and undermining vaccination programs before and during a deadly measles outbreak in Samoa in 2019. In particular, two attempts to do this have really irked me. The first comes from a predictable source, the Brownstone Institute, in the form of an article by David Marks entitled RFK Jr. and the Samoan Measles Outbreak. The second shows just how far a certain oncologist and EBM methodolatrist turned COVID-19 contrarian and public health underminer has fallen. Obviously, I’m referring to Dr. Vinay Prasad, who recently posted to his monetized Substack one of the most risibly historically ignorant attempts at gaslighting RFK Jr.’s role in the 2019 Samoan measles outbreak that I’ve yet seen, entitled The true story of the Samoa measles outbreak. (Hint: It ain’t.) Either that, or it was intentional faux ignorance. You be the judge after this post. I’m also amused at how someone like Dr. Prasad, who attacks any lack of sourcing, has barely sourced his little post, having apparently relied on a single article from an obscure journal. At least, that’s the only source he cites.
As you will see, these defenses of RFK Jr. tend to rely heavily on the fact that the low uptake of the measles-mumps-rubella (MMR) vaccine had occurred as a result of a tragic error that had led to the MMR-related deaths of two one-year-old children. The central argument seems to boil down to this: The low MMR uptake that predisposed the island to a measles outbreak wasn’t RFK Jr.’s fault (sort of true, but incomplete, as RFK Jr. added fuel to the antivax fire after news of the babies’ deaths were reported). The intended implication is, of course, that RFK Jr.’s opportunistic support of antivaxxers on the island in the middle of the outbreak, plus his use of the Kennedy name to promote antivax misinformation about MMR to the highest levels of government in Samoa, were no big deal because they weren’t the primary cause of the outbreak.
Buckle up, this is going to be a long one, even by my standards.
The gaslighting begins: The origins of low MMR uptake on Samoa
The term “gaslighting” comes from the title of the 1944 American film Gaslight, which was based on the 1938 British theatre play Gas Light by Patrick Hamilton, although the term didn’t become widely used until the last decade or so. In the film, the husband, played by Charles Boyer, emotionally manipulates his wife (played by Ingrid Bergman) to make her doubt her own grasp of reality—and even her sanity—so that he could steal from her. He does this by isolating his wife and using various trickery and emotionally abusive techniques to make her question reality. The title of the film refers to one example of the husband’s deceptions, the gaslight illumination of the couple’s house that seems to dim and flicker whenever the husband leaves his wife alone at home. When she asks him, “Why do the lights keep flickering?” he responds that he doesn’t know what she’s talking about and insists that the lights are not flickering, that it’s just her imagination. Since its wider adoption in more recent years the meaning of “gaslighting” has broadened beyond describing emotional abuse designed to make a person question her memory and reality to refer to the use of misinformation and propaganda to produce a false narrative about the past in order to manipulate a population. Given how horrible RFK Jr.’s behavior was stoking antivaccine fears in the middle of a deadly epidemic on Samoa, just months before the COVID-19 pandemic hit, you can see why his apologists would want to gaslight you about his role there, and they have been furiously gaslighting ever since his nomination for HHS Secretary—since even before his nomination, actually.
As I read the two articles trying to absolve RFK Jr. of any responsibility for his antivaccine proselytizing on Samoa from June 2019, three months before the deadly measles outbreak began, through early 2020, after dozens of children had died and over 5,000 had been sickened, I noticed that Marks and Dr. Prasad take different tacks. I’ll start with Dr. Prasad, whose central argument seems to be that it wasn’t RFK Jr.’s fault because one of the main reasons why MMR uptake had fallen so low right before measles was introduced by a person suffering from the disease arriving in Samoa on a flight from New Zealand in August 2019, was a tragic medical error involving reconstituting MMR vaccine that had resulted in the deaths of two babies. This is, again, true enough but irrelevant to the question of just how awful RFK Jr. behaved after that incident, including during the deadliest weeks of the measles outbreak. The overall facts and timeline are not in dispute, either. The story of the Samoan measles outbreak has also been widely reported by many reputable sources, not the least of which is Brian Deer, author of The Doctor Who Fooled the World and the investigative journalist who first reported on antivax gastroenterologist Andrew Wakefield‘s research fraud and conflicts of interest in his study linking MMR vaccination to “autistic enterocolitis.” Predictably, Dr. Prasad spends the vast majority of his article harping on the tragic accident that fueled a downward spiral in MMR uptake the year before the outbreak and takes a “What, me worry”? attitude towards RFK Jr.’s activities on Samoa afterward. Spoiler alert: While there was plenty of blame to go around for this deadly debacle, including on the part of the Samoan government, just because the causes of the outbreak on Samoa were multifactorial does not absolve RFK Jr. from doing his damnedest to make things worse and kill more babies.
Before I dig in, I also can’t help but mention that I first noted Dr. Prasad becoming—shall we say?—receptive to the sort of antivax misinformation that RFK Jr. has spent the last two decades using the Kennedy name to promote when he expressed agreement with some of RFK Jr.’s claims made during an appearance on Joe Rogan’s podcast in 2023, when he agreed with RFK Jr.’s deceptive “criticism” of the birth dose of the hepatitis B vaccine and suggested that an unethical “multi-arm factorial RCT” (randomized controlled clinical trial) of the entire childhood vaccination schedule might be a good idea. Basically, Dr. Prasad had swallowed whole RFK Jr. and his lawyer Aaron Siri’s deceptive insinuation that, because not every single last vaccine in the childhood vaccination schedule had been tested in an RCT with a saline placebo control, then the entire vaccine schedule was suspect. It’s a bogus argument based on a half-truth for many reasons, not the least of which are that (1) it would be unethical to test new versions of existing vaccines in a placebo-controlled RCT because that would leave the control group unprotected against the disease for which the vaccine was designed; (2) all the original versions of the vaccines in the childhood schedule were tested against saline or an appropriate control; and (3) saline isn’t always the correct control. At the time, I also noted that a “multi-arm factorial RCT” of the childhood vaccination schedule that would not be feasible or ethical but would require hundreds of thousands or millions of participants. In his EBM methodolatry, Dr. Prasad seemed…unconcerned.
Ultimately, Dr. Prasad’s audience capture that led him to credulously parroting old antivax talking points as though they were anything but old antivax talking points got worse, with him ultimately even embracing a very old antivax message of “do not comply” with COVID-19 vaccine mandates. More recently, he has been rushing to kiss RFK Jr.’s posterior and support his agenda, while trying to pretend that RFK Jr.’s “inconvenient” antivax stances didn’t exist or are just minor forgivable peccadillos, nothing compared to the supposed righteousness about chronic disease, nutrition, and attacks on the pharmaceutical industry. The one source article that Dr. Prasad cites is entitled A Perfect Storm: The Social and Institutional Contexts of Samoa’s 2019-2020 Measles Epidemic and the Lessons learned for the COVID-19 Pandemic. Published in October 2020 in the The Journal of Samoan Studies, two of whose authors are scholars living and working in Samoa, it states its purpose and methods thusly:
Through a combination of personal observation, analysis of media articles, government reports and historical documents, we present an overview of the circumstances of the measles epidemic. We trace the circumstances of low vaccination coverage, institutional weaknesses and an uninformed public resulting in a delayed an effective response. In conclusion we reflect on the lessons that history offers on public health services in Samoa.
Fair enough, but it also crows about how, by October 2020, Samoa had learned its lesson and successfully kept COVID-19 out:
Samoa remains one of the few countries in the world with no confirmed cases of Covid 19, a pandemic which has affected millions and killed thousands across the world. Developing countries have been identified as being extremely vulnerable to the impact of Covid 19 due to limited testing capabilities and weak health systems. The vulnerability of Samoa to an outbreak was most evident after the devastating impact of the measles outbreak in 2019 and the lessons learned from it have not been forgotten. Samoa implemented a sweeping series of restrictions in travel, improved health education about Covid 19 and a state of emergency swiftly. By these means, a country which still does not have testing capabilities and which has limited health resources has been able to prevent Covid 19 reaching its shores.
Funny how, given his opposition to “lockdowns,” masking, and non-pharmaceutical interventions to slow the spread of COVID-19, Dr. Prasad left that part out, which was kind of the entire point of the article. In any case, I can see why he likes this article. Although it does mention the problem of antivax disinformation, it mentions RFK Jr. not at all. No wonder he wrote an article like The true story of the Samoa measles outbreak.
Dr. Prasad begins:
Many commenters link RFK Jr to an outbreak of measles in Samoa that killed more than 80 children. What actually happened? And who is at fault?
I had a chance to brief myself on the facts of the case and this is my summary.
Measles was not present on Samoa till brought by visitors in the 1880s.
In July 2018, two nurses killed two kids with the MMR shot when they drew it up with expired atacurium (a paralytic) rather than saline. They took the vials home and hid them, realizing their mistake. They would be convicted in 2019 for manslaughter.
The phrase “I had a chance to brief myself on the facts of the case” is doing a lot of heavy lifting here. Apparently he read one article that supported (somewhat) his preexisting desire to absolve RFK Jr. of any guilt for adding fuel to the fire of the antivaccine views that had rendered Samoa vulnerable to such a horrific measles outbreak. I was also wondering just what the heck the relevance was of measles not having been present on Samoa until 140 years ago. Apparently Dr. Prasad can read Wikipedia too.
In any case, it is true that the inciting event that sparked the fears that led to low MMR uptake and led to the Samoan government halting the distribution of MMR for ten months was the deaths of two infants due to a horrific, tragic mistake by two nurses, who later were ultimately convicted of negligent manslaughter. An account of the trial in a Samoan newspaper can be found here:
According to police facts tendered in court, standard procedures for preparing vaccines were not followed at the Tuasivi Hospital on the morning of the incident, including a requirement that registered nurses thoroughly check the labels on the components used to mix vaccines.
Luse mixed the M.M.R. vaccine powder with an expired anaesthetic, the Court was told.
“Unfortunately Luse, without checking the vial, mixed the powder of vaccine with what she thought was a proper [substance for dilution],” the facts state.
“It was not.”
Justice Vui found that the vial containing anaesthetic was clearly labelled but not checked.
“That action would have avoided the tragic events that were then followed,” he said.
“[Luse] breached protocols and became grossly negligent in the discharge of her duties.”
The fatal vaccination was performed by a trainee nurse under Luse’s supervision with the syringe and ampule discarded in a rubbish bin.
But the baby’s mother, soon after leaving the clinic with her infant daughter, began to notice rapid changes to her baby while waiting for a bus home.
“Her baby’s body felt cold; her eyes could not open properly and her legs were [spasming] out; she rushed back to the Hospital for assistance and the nurses, including the defendants, tried to revive the baby but the young baby stood no chance,” Justice Vui said.
“She passed away.”
I cite this mainly to demonstrate that, yes, it was definitely a horrific negligent act that killed two children that sparked the suspicion and fear of the MMR vaccine in Samoa—understandably so. And, yes, initially the cause of the deaths wasn’t known. (Dr. Prasad points to a contemporaneous headline, “Two babies die in Samoa hospital minutes after receiving ‘MMR’ vaccinations; Investigation underway.”) And, yes, the medication error wasn’t discovered for two weeks, which, according to Dr. Prasad’s source, led to fear and suspicion of the MMR vaccine itself:
There was an immediate presumption that the vaccine itself was responsible for the deaths, and it was announced in the press that the vaccine was withdrawn. Two weeks passed before health authorities discovered that the infants had been poisoned; the two nurses involved, realizing their error, had taken the vials home and hidden them. However this was not made public. During the intervening period, there was intense speculation in the media in Samoa and abroad about whether the vaccine itself had caused the deaths.
Worse:
These and other reports planted the suspicion firmly in the minds of the public that the MMR vaccine was the cause of the deaths. Although there was an immediate four-month suspension of the administration of the MMR vaccine and although ten months passed before routine vaccinations resumed, with the public still mostly unaware that there had been a medical misadventure, there was widespread public fear of the MMR vaccine. Several mothers were reported as saying they had lost faith in the public health system they preferred to treat illnesses via traditional means (Tautua- Fanene 2018). The suspicion that the vaccine was to blame enabled anti-vaccination activists in Samoa and overseas to seize public attention.
I must admit that I am not entirely buying the claim in this article that Samoans had been “mostly unaware that there had been a medical misadventure.” It didn’t take much searching to find news stories before that discussing the case, such as this one from November 2018 reporting that the inquest into the MMR vaccine as the cause of the babies’ deaths had been stayed pending the outcome of the trial of the two nurses accused of the deadly mixup. Indeed, the Samoan Ministry of Health’s own annual for 2018/2019 states:
In August 2018, Cabinet instructed a Commission of Inquiry to investigate the deaths of the two babies who passed away due to the Mumps, Measles & Rubella (MMR) Vaccinations carried out at the Safotu District Hospital. The Commission members were Judge Tuiloma Neroni Slade as Chair, Leoo Dr John Adams and Lealaiauloto Liai Siitia as Commission members. Public hearings were conducted in September 2018 whilst the Criminal proceedings for the alleged Nurses were being held.
Even with this additional background, in fairness, I have to conclude that it does appear to be true that the Samoan government took way too long after it had discovered the problem that led to the babies’ deaths after vaccination to inform the public. Australian physician Prof. David Isaacs noted in a brief communication to The Journal of Paediatrics and Child Health:
The Government suspended the MMR immunisation programme after the July administrative error. The cause of this vaccine tragedy was not made public for months, even after re-starting MMR vaccine in November 2018. In July 2019, two nurses were sentenced to 5 years’ prison for inadvertently using a curare-like muscle blocking agent instead of water to dilute lyophilised (powder) MMR vaccine. This sort of disaster is not new: 15 infants died in northern Syria in 2014 when atracurium was used as a diluent instead of water.6 It is unclear why muscle relaxants were kept in immunisation facilities in Syria or Samoa.
I feel a need for a quick aside here: WTF? No seriously, WTF? How can something like this have happened not once, but twice? Apparently, in Syria, instead of the regular diluent for the vials, the MMR was mixed it with atracurium, which has the same color bottle and same patch on it. “WTF?” indeed.
Moving on, yes, in 2018 a tragic act of negligence caused the deaths of two babies after receiving the MMR vaccine, and, yes, the Samoan government appears to have been way too secretive about what it knew and when it knew it. As we know, whenever there is a deficit in information about a tragedy involving a vaccine, antivaxxers and conspiracy theorists will always leap in to fill the void with rampant speculation and misinformation. That is exactly what happened and exactly what RFK Jr. and his minions did their best to contribute to. Dr. Prasad blithely describes what happened thusly:
Did some local activists seize upon the deaths to discourage vaccination? Possibly, but that is inevitable. After any tragedy some people will discourage exposure. I know someone who advises against moving walkways because they read about a woman whose leg got caught. Chipotle famously had a huge drop in business after an E.coli outbreak. Often these responses are disproportionate– more than rational. Naturally, Samoans, who are often poor with low health literacy, would be quick to drop MMR vax after someone died. But notably this was sanctioned by the government.
This is a Bizarro World description of what really happened. For one thing, there is no “possibly” about it. Local antivaxxers did seize upon the incident to spread antivax misinformation and disinformation. Indeed, the antivax organization founded by RFK Jr., Children’s Health Defense, lionized one such local antivax activist with whom it had worked, Edwin Tamasese, who had been arrested for advocating quackery (claiming that vitamins A and C alone could cure measles) and spreading misinformation. RFK Jr. himself wrote an introduction to the article, in which he lauded Tamasese as a “leading Samoa medical freedom hero” and after which Tamasese was given a lot of digital space to tell his side of the story, which included touting a protocol that he had adapted from antivax physician James Meehan and claiming that the mass vaccination campaign undertaken during the outbreak “statistically” had had no effect on the outbreak’s course. Make no mistake, CHD and RFK Jr. were tight with local Samoan antivax leaders like Tamasese. Indeed, according to RFK Jr. himself:
Medical freedom advocates around the globe know Edwin Tamasese’s name. In June 2019, I visited Samoa at the invitation of Prime Minister Tuilaepa Lupesoliai Neioti Aiono Sailele Malielegaoi who has served as the Prime Minister of Samoa and Leader of the Human Rights Protection Party since 1998.
I went to Samoa to attend an independence celebration and discuss with the government the introduction of a medical informatics system that would allow Samoa’s health officials to assess, in real time, the efficacy and safety of every medical intervention or drug on overall health.
Edwin Tamasese had arranged the trip and Children’s Health Defense had offered to finance the innovative system. Samoa banned certain vaccinations after several children had died following MMR vaccines the previous year.
I can’t resist quoting Marks at Brownstone again, because he himself cites Tamasese’s attempts to blame the vaccine for people getting sick:
While the press condemned him as an anti-vaxxer, Tamasese’s interventions and observations are revelatory. In an interview after the outbreak subsided, he said, “We were very careful to take statistics when we were going in to try to identify trends. When we assessed our numbers, 98 percent of those who were getting ill had been vaccinated consistently six to seven days prior to illness. The excuse was that the vaccine did not have time to become effective. However, according to an immunologist on the team, the six to seven-day period was also the length of time it would take an under-attenuated vaccine to make the recipient sick.”
I wonder if Dr. Prasad thinks that the MMR vaccine can do this. Certainly, RFK Jr. seemed to agree that it could, as you will see. Certainly, these children could have caught measles during the window between vaccination and the development of levels of protective antibody sufficient to prevent and attenuate disease, but, as is usual, antivaxxers blamed the illness on the vaccine. Again, remember that Tamasese invited RFK Jr. to Samoa and that CHD championed him after he had been arrested for spreading antivax propaganda and using vitamins to treat patients with measles. Nor was Tamasese alone in exulting over a visit to Samoa by his antivax hero. Another Samoan antivaxxer, Taylor Winterstein, posted a lot on Instagram:
Lest you doubt my assertion that Ms. Winterstein is antivaccine, here is another Instagram post by her:
Note the common antivaccine trope that it is “bullying” to criticize antivaxers for refusing to vaccinate or for spreading antivaccine misinformation. In this post, she invokes Nuremberg, a favorite misapplication of the Nuremberg declaration beloved of antivaxers ranging from Barbara Loe Fisher to Rob Schneider to, well, RFK Jr. himself, complete with tropes about “informed consent” (which in the hands of antivaxers is really misinformed refusal, in which a decision is made based on massively exaggerated or made up risks, made up “toxins,” and a massive understatement of benefits):
Elsewhere, Winterstein also referred to the government effort to vaccinate its population as “NaziSamoa.”
These are but a few of the many reasons why these events do not absolve RFK Jr. and Samoan antivaxxers who looked to him for guidance. They made the situation so much worse the following year through their spreading of antivax propaganda. All of these things can be true at the same time, and the fact that a tragically negligent error caused two deaths that provoked fear among Samoan parents and that the Samoan government was less than forthright about what it knew does not absolve RFK Jr. Moreover, Dr. Prasad’s comparison of people being afraid of the MMR after the deaths of two children to a woman afraid of moving walkways after getting her leg caught in one or to the Chipotle E. coli outbreak is insultingly stupid, obviously intended to downplay the tsunami of misinformation that arrived from outside antivaxxers to bolster the local antivaxxers as no big deal and to dismiss the fears of the Samoan population after the babies’ deaths as overblown, but human nature that would have occurred regardless of the activities of local antivaxxers and their foreign patrons at CHD led by RFK Jr.
The single worst part of the passage above is where Dr. Prasad cluelessly states:
What did RFK say in Samoa? I don’t know but the time course makes no sense. He visited in 2019, but vax rates were already low. The die had been cast.
Dr. Prasad’s argument here seems to be: Things were already so bad that RFK Jr.’s activities didn’t matter. However, we already know that they did matter. We know, for instance, that in 2018 CHD had been spreading antivax misinformation blaming the MMR vaccine for the two babies’ deaths and that it didn’t update or change the social media posts spreading that message after the story of the medication error hit the news. Moreover, we know what he said. He reinforced and supported people like Edwin Tamasese and Taylor Winterstein, and we know local antivaxxers like them were saying. We also know that RFK Jr. wrote a letter to Samoan Prime Minister Tuilaepa Aiono Sailele Malielegaoi about the MMR and measles in the middle of the outbreak.
RFK Jr. just wrote me a letter
I have a copy of that letter to Samoan Prime Minister Prime Minister Tuilaepa Aiono Sailele Malielegaoi and wrote about it at the time, alas not on SBM. The letter was dated November 19, 2019, right smack dab in the middle of the deadliest weeks of the epidemic. We know what it said. Its existence and content were reported fairly widely in the mainstream press (e.g., The Washington Post). None of this is at all difficult to discover for anyone who actually looks, but oddly enough, Dr. Prasad apparently appears not to have bothered his planet-sized brain to try, instead just throwing up his hands and saying, in essence, “Who can possibly know what RFK Jr. said and did on Samoa then?” It’s such disingenuous bullshit, so easily debunked, that I was surprised that even someone like Dr. Prasad would publish it. The contempt that Dr. Prasad shows for his audience is palpable.
Just to rub it into Dr. Prasad’s face, let’s take a look at RFK Jr.’s actual letter, which I conveniently decided to post as images:
Interestingly, David Marks at Brownstone approvingly cites this letter, even providing a link to it, lest antivax conspiracy theorists think that I forged the letter or something. Marks actually quite likes the letter and thinks that it reflects well on RFK Jr. (it doesn’t):
In November 2019, while the deaths of Samoan children were rapidly increasing, Kennedy wrote a comprehensive letter to the Samoan Prime Minister, presenting some possible causes of the unprecedented, virulent outbreak of measles. His concerns about the epidemic in Samoa highlight striking anomalies that were apparent to a few investigators at the time, although they remain unexplained.
Hint: As you have no doubt guessed (and as I will explain), these “anomalies” cited by RFK Jr. were not actually anomalies at all, nor do they “remain unexplained.” Since I know that Dr. Prasad, planet-sized brain or not, master of EBM or not, will never bother to critically examine the actual content of RFK Jr.’s letter (of whose existence he was apparently conveniently unaware; that is, if you believe he was actually unaware, which I’m not sure that I do), I will. To do so, I have modified and condensed a discussion of the letter that I wrote contemporaneously, when news of this letter first hit the media.
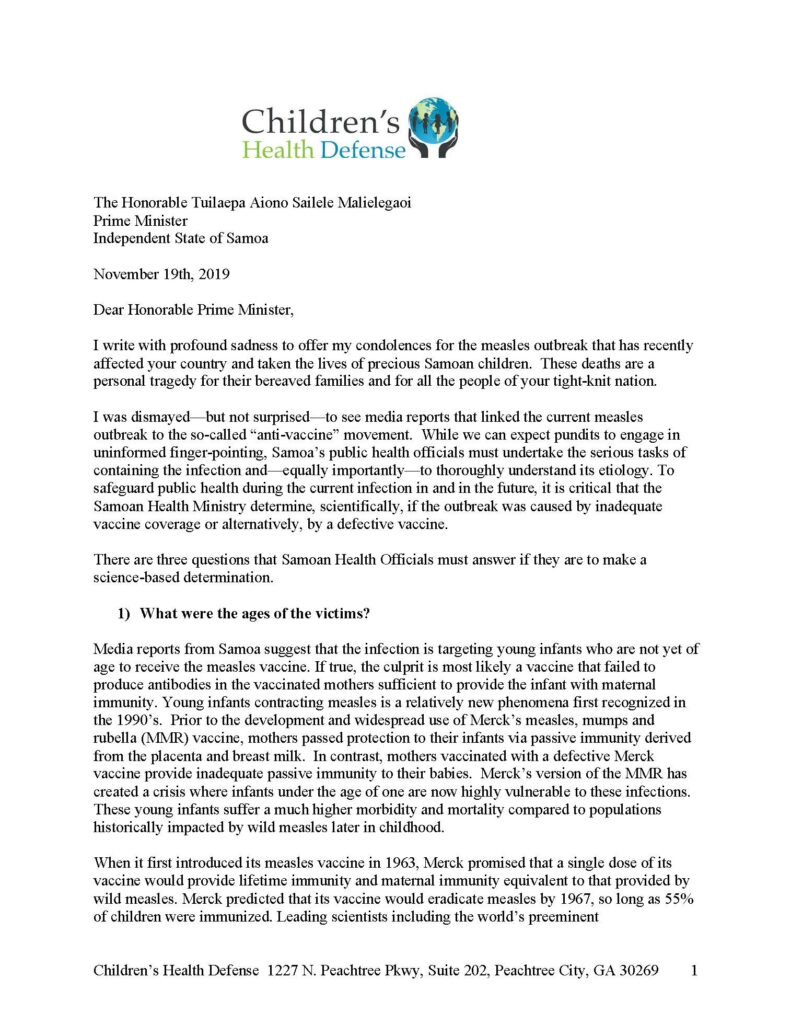
RFK Jr.’s letter begins:
I write with profound sadness to offer my condolences for the measles outbreak that has recently affected your country and taken the lives of precious Samoan children. These deaths are a personal tragedy for their bereaved families and for all the people of your tight-knit nation.
I was dismayed—but not surprised—to see media reports that linked the current measles outbreak to the so-called “anti-vaccine” movement. While we can expect pundits to engage in uninformed finger-pointing, Samoa’s public health officials must undertake the serious tasks of containing the infection and—equally importantly—to thoroughly understand its etiology. To safeguard public health during the current infection in and in the future, it is critical that the Samoan Health Ministry determine, scientifically, if the outbreak was caused by inadequate vaccine coverage or alternatively, by a defective vaccine.
There was, of course, no evidence that the outbreak in Samoa had anything whatsoever to do with a “defective” vaccine. RFK Jr. was just pulling this bit right out of his nether regions. Moreover, when you have vaccine uptake well south of 50% (As you’ve seen, MMR uptake right before the outbreak started was estimated to have fallen to around 31%), measles outbreaks can happen. In the background of low vaccine coverage (particularly as low as it was in Samoa before the outbreak), one case coming in from another country can rapidly become hundreds and then thousands of cases.
After that inauspicious and disingenuous introduction, RFK Jr. asked three questions:
- What were the ages of the victims?
- Were Samoa’s fatal measles cases caused by strains of measles not targeted by Merck’s vaccine?
- Were the fatal Samoan infections from a vaccine strain?
Let’s take on #1 first. What was RFK Jr. playing at? Nothing good:
Media reports from Samoa suggest that the infection is targeting young infants who are not yet of age to receive the measles vaccine. If true, the culprit is most likely a vaccine that failed to produce antibodies in the vaccinated mothers sufficient to provide the infant with maternal immunity. Young infants contracting measles is a relatively new phenomena first recognized in the 1990’s. Prior to the development and widespread use of Merck’s measles, mumps and rubella (MMR) vaccine, mothers passed protection to their infants via passive immunity derived from the placenta and breast milk. In contrast, mothers vaccinated with a defective Merck vaccine provide inadequate passive immunity to their babies. Merck’s version of the MMR has created a crisis where infants under the age of one are now highly vulnerable to these infections. These young infants suffer a much higher morbidity and mortality compared to populations historically impacted by wild measles later in childhood.
First of all, passive immunity to a disease like measles doesn’t come primarily from breast milk. It comes from the IgG antibodies passed to the infant through the placenta into the blood. Thus is immunity to diseases the mother has had passed on to the baby for a time. At term, dependent on the immunological experience of the mother, placental transfer allows the newborn to acquire different specificities of IgG antibodies. This results in an identical recognition pattern of antigens between the mother and her offspring. After birth, the baby receives no further IgG antibodies that can result in measles immunity from the mother, and levels of IgG antibodies in the infant wane to zero by between 6-12 months of age. The antibodies in the breast milk consumed by the baby are primarily secretory IgA, a class of antibody that is adapted to resist digestion by the GI tract and that serves primarily to protect the mucosal surfaces (e.g., mouth, nasal passages, etc.) from environmental pathogens. There are antibodies to measles in milk, but, contrary to the myth that breast feeding can protect against measles, in a study of Nigerian women and their infants the level of measles-specific antibodies in milk dropped below the protective level within two weeks of birth.
But what about antibody levels in babies born to mothers who had natural immunity to measles versus those born to mothers who had been vaccinated against measles? A 2010 study sought to answer that question in 207 mother-infant pairs in Belgium, measuring serum IgG antibody level over the first twelve months of life in women who had natural immunity to measles and comparing those levels to what was observed in mothers vaccinated against the measles. These investigators reported the already known and accepted result that at birth babies born to vaccinated mothers have significantly lower anti-measles antibody titers than babies born to mothers with natural immunity. However, here’s the key sentence: “At 6 months of age, more than 99% of infants of vaccinated women and 95% of infants of naturally immune women had lost maternal antibodies according to the model.”
Basically, high vaccine uptake is the best way to protect these infants, coupled with earlier vaccination during outbreaks. If herd immunity is high, faster waning of immunity due to maternal antibodies is much less of a problem. If herd immunity is not high, then vaccinating earlier is a viable option to protect these infants. I also must repeat that there was (and is) no evidence that the vaccine was defective.
An earlier review of the literature found that, yes, antibody level does tend to start out lower and wane to lower than needed for protection against measles in the children of vaccinated mothers compared to children of mothers with natural immunity, although not all studies showed a difference. The whole issue is, as you might expect, way more complicated than RFK Jr. lets on. For example, part of the reason that the first dose of MMR isn’t recommended before age 12 months is because the persistence of maternal antibodies can interfere with the generation of an immune response to the vaccine. However, in nations with high vaccination rates, waiting until 12 months of age to administer the first dose of MMR is not a problem, due to herd immunity. Also, although it might blunt an immune response to vaccine, persistence of maternal antibodies doesn’t prevent an immune response. That’s why the CDC was recommending at the time that during an outbreak health departments should consider vaccinating children earlier than the recommended age of first dose in a non-outbreak situation and that they should also consider giving an additional booster to children.
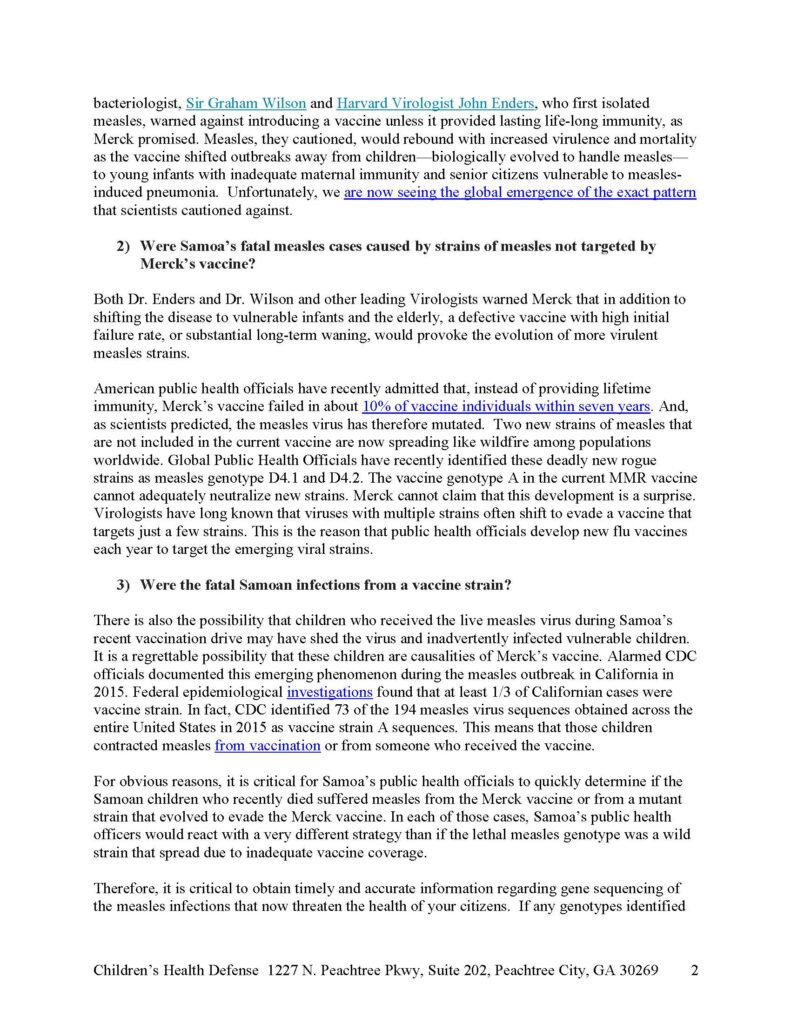
I must admit that I laughed out loud at this passage:
When it first introduced its measles vaccine in 1963, Merck promised that a single dose of its vaccine would provide lifetime immunity and maternal immunity equivalent to that provided by wild measles. Merck predicted that its vaccine would eradicate measles by 1967, so long as 55% of children were immunized. Leading scientists including the world’s preeminent bacteriologist, Sir Graham Wilson and Harvard Virologist John Enders, who first isolated measles, warned against introducing a vaccine unless it provided lasting life-long immunity, as Merck promised. Measles, they cautioned, would rebound with increased virulence and mortality as the vaccine shifted outbreaks away from children—biologically evolved to handle measles— to young infants with inadequate maternal immunity and senior citizens vulnerable to measles-induced pneumonia. Unfortunately, we are now seeing the global emergence of the exact pattern that scientists cautioned against.
I do like how RFK Jr. pointed to nearly 60-year-old predictions by scientists, who clearly vastly underestimated the level of herd immunity necessary to keep measles in check in a population and likely didn’t envision how easily diseases can now jump borders, thanks to air travel, tourism, and people traveling to visit their families, over 55 years later. It’s a classic “science was wrong before” bit of misdirection. I also counter by pointing out that lifelong immunity can be provided with the help of booster vaccines.
Next, RFK Jr. made this whopper of a claim:
Both Dr. Enders and Dr. Wilson and other leading Virologists warned Merck that in addition to shifting the disease to vulnerable infants and the elderly, a defective vaccine with high initial failure rate, or substantial long-term waning, would provoke the evolution of more virulent measles strains.
American public health officials have recently admitted that, instead of providing lifetime immunity, Merck’s vaccine failed in about 10% of vaccine individuals within seven years. And, as scientists predicted, the measles virus has therefore mutated. Two new strains of measles that are not included in the current vaccine are now spreading like wildfire among populations worldwide. Global Public Health Officials have recently identified these deadly new rogue strains as measles genotype D4.1 and D4.2. The vaccine genotype A in the current MMR vaccine cannot adequately neutralize new strains. Merck cannot claim that this development is a surprise. Virologists have long known that viruses with multiple strains often shift to evade a vaccine that targets just a few strains. This is the reason that public health officials develop new flu vaccines each year to target the emerging viral strains.
I recognized this nonsense right away as having come from Andrew Wakefield and his risible speculation about an impending “sixth extinction” due to the evolution of resistant measles mutants due to—you guessed it!—vaccines. Thankfully for purposes of keeping this post from ballooning to 10,000 words, I dealt with Wakefield’s incompetent attempted prestidigitation with facts and science five years ago. You can read the whole piece if you want the gory details of this particularly unscientific and brain-dead bit of antivaccine propaganda. Suffice to say that RFK Jr. was basically channeling some particularly deranged latter day Wakefield antivax propaganda in the passage above. I wonder if Dr. Prasad recognized that? Of course he didn’t. Remember, before the pandemic he thought that dealing with antivax misinformation was so trivial as to be not worth engaging his massive intellect.
Let’s look at RFK Jr.’s final question for Prime Minister Tuilaepa Sailele Malielegaoi:
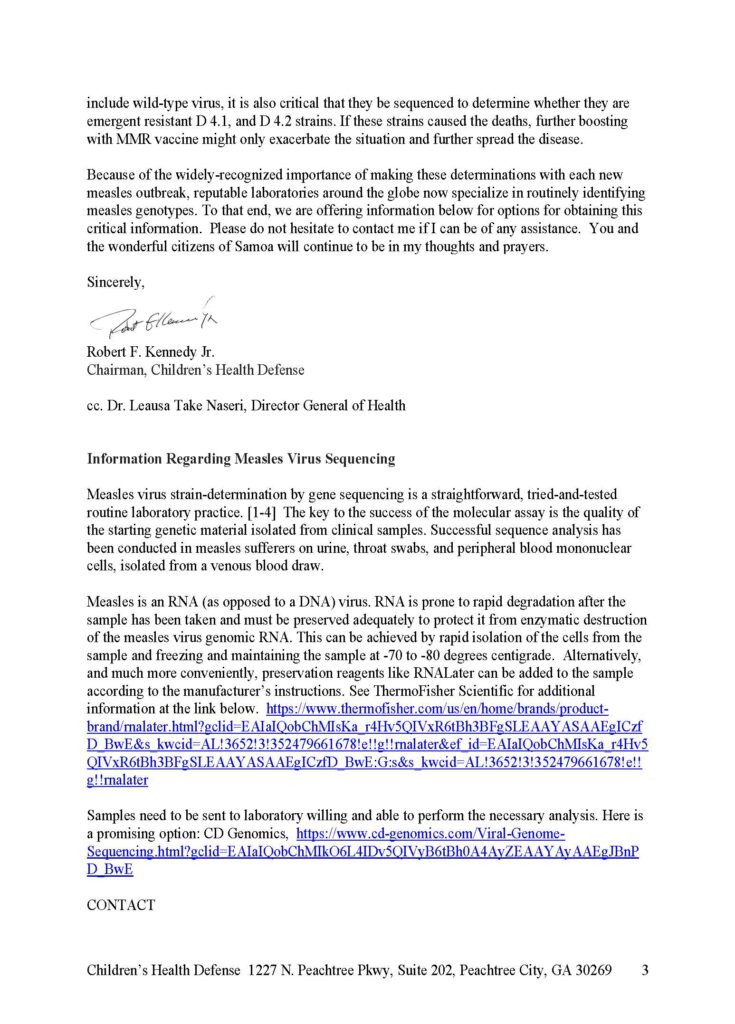
There is also the possibility that children who received the live measles virus during Samoa’s recent vaccination drive may have shed the virus and inadvertently infected vulnerable children. It is a regrettable possibility that these children are causalities of Merck’s vaccine. Alarmed CDC officials documented this emerging phenomenon during the measles outbreak in California in 2015. Federal epidemiological investigations found that at least 1/3 of Californian cases were vaccine strain. In fact, CDC identified 73 of the 194 measles virus sequences obtained across the entire United States in 2015 as vaccine strain A sequences. This means that those children contracted measles from vaccination or from someone who received the vaccine.
For obvious reasons, it is critical for Samoa’s public health officials to quickly determine if the Samoan children who recently died suffered measles from the Merck vaccine or from a mutant strain that evolved to evade the Merck vaccine. In each of those cases, Samoa’s public health officers would react with a very different strategy than if the lethal measles genotype was a wild strain that spread due to inadequate vaccine coverage.
RFK Jr. was either lying or just misinforming Prime Minister Tuilaepa Sailele Malielegaoi. There were no vaccine strain measles cases in the Disneyland outbreak. All measles cases in that outbreak were caused by wild-type measles. The claim that “vaccine shedding” can cause measles outbreaks is not scientifically supported. It is, in fact, utter nonsense. Again, there are only two possibilities. Either RFK Jr. was utterly clueless but didn’t care, or he knew and was lying. Again, take your pick. That he would have the temerity to write such a letter to Prime Minister Tuilaepa Sailele Malielegaoi, who’s struggling to lead a small, underdeveloped country through a major crisis, says a lot about RFK Jr.’s character, none of it good. So does his characterization of a measles outbreak that sickened over 5,000 and ultimately killed 83 children as “mild.” Come to think of it, Dr. Prasad claiming that he didn’t know what RFK Jr. said and did before and during the Samoan measles outbreak says a lot about his character, none of it good.
Basically, Dr. Prasad’s whole apologia falls for the plausible deniability that RFK Jr. has long cultivated thusly:
The Samoa episode fits Kennedy’s M.O. As an anti-vax champion, he has decried vaccinations as unsafe and ineffective—repeating the debunked notion that vaccines cause autism—and he has boosted attempts throughout the world to convince people to eschew vaccines. Yet when he has been questioned critically about these efforts, he has issued false denials and contended that he’s just raising questions and calling for more research. In July 2023, at the invitation of House Republicans, he appeared at a congressional hearing and declared, “I have never been anti-vax. I have never told the public to avoid vaccination.” Yet that same month, during a podcast interview, he asserted, “There’s no vaccine that is safe and effective.”
Kennedy, as he claimed in the interview for Shot in the Arm, may not have publicly urged Samoans to refuse the measles vaccine. But he encouraged those who did, and the group he led helped spread misinformation to discredit vaccinations there. After the tragedy was over, he dismissed the outbreak as not serious and extolled the anti-vaxxers who helped bring it about.
This is what RFK Jr. does. it’s what he’s always done. It’s what he’s likely to continue to do whether he’s confirmed as HHS Secretary or not. There’s a reason why I periodically feel obligated to remind everyone that RFK Jr. is not a “vaccine skeptic” or “pro-safe vaccines,” but “antivaccine,” along with receipts. Unfortunately, Dr. Prasad is apparently not satisfied with just gaslighting RFK Jr.’s role in contributing to make this whole debacle so much worse. Just wait until you his conclusion. First, however, Brownstone’s gonna Brownstone. Let’s take a look.
Brownstone does what Brownstone always does: promote antivax propaganda
Dr. Vinay Prasad’s article is quite bad, but it’s of a piece with the Brownstone article by David Marks. One area where they both strike the same note is in disingenuously wondering why the mortality rate of measles was so high during the Samoa outbreak. Dr. Prasad, for instance, takes a very brief paragraph to say:
And what about the high death rate? Ultimately the case fatality rate for measles was very high. That feels like iatrogenic harm (with inappropriate therapy) or there are serious limitations to the health system. Both of these are true.
“Iatrogenic harm”? I’m confused here. The term “iatrogenic harm” implies that the harm was caused by doctors, by conventional medicine. While it is true that quacks like Edwin Tamasase were peddling vitamins as treatment for measles and that a lot of Samoans were turning to folk medicine and traditional healers to treat measles, Dr. Prasad cites no evidence to support this claim of iatrogenic harm. It is, however, true that the fatality rate for measles in this outbreak was unusually high. Generally, we cite an estimated mortality rate for measles of around 1 in 1,000 cases, while in Samoa by the Christmas holiday in 2019 there had been 79 deaths from 5,520 cases, with a mortality rate of approximately 14 per 1,000 cases, which was truly alarming. It is certainly true that poverty and lack of access to proper medical care, plus distrust of medical authorities, did indeed form the “perfect storm” (to quote the title of the article that seems to have been Dr. Prasad’s only source for his article) resulting in many more deaths than would have resulted from a comparable-sized outbreak in a developed nation.
On the ground, public health workers knew what was happening:
And in developing countries, the suffering from measles is always worse. Many rural Samoans had no transport, feared going to hospital, or tried traditional healers first. By the time people did bring their babies in, they were extremely sick, said Australian anaesthetist Dr Dan Holmes, who led the Australian emergency medical team and was among more than 100 medical personnel deployed to Samoa in the thick of the epidemic.
He spent two “relentless” weeks trying to save babies with complications from measles including pneumonia, collapsed lungs, dehydration, and brain inflammation.
“Your day might start at 6am with a baby who is unconscious and not breathing, and you might lose that baby, then there’s another one, day after day,” Holmes said. “It’s impacted me more than anything I’ve done. It makes me feel so angry that it could have been prevented.”
Me, too, Dr. Holmes. Me, too. I’m particularly angry and alarmed that the man who abused his family name and fame to facilitate the spread of antivaccine misinformation during the pandemic is now poised to be put in charge of the department responsible for administering the non-military health programs of the federal government.
Meanwhile, Brownstone flack Marks does what Brownstone flacks do. He Gish gallops:
A renewed effort to vaccinate with this alternate supply began in the first week of December 2019; it was hailed as the reason the outbreak subsided. Measles vaccines take at least 10 days before creating an immune response. There has been no explanation for the data confirming that the onset of cases dropped dramatically two weeks before this vaccination drive could have had any effect.
Next up:
Any considered analysis of the accessible facts soundly contradicts the conjecture that the high death count was related to low vaccination rates. News coverage continues to rely on a UNICEF report estimating the vaccination rate of one-year-olds was as low as 31% as the epidemic started. However, the Samoan Government Health Ministry reported (p. 9) in June 2019 — three months before the measles outbreak began — that 80% of 12-month-old babies had received the MMR vaccine.
Even if the above is accurate, I note that 80% uptake is still far below the necessary 90-95% uptake required for herd immunity to measles in a population. Also, Marks does realize that epidemics peak and then subside on their own, doesn’t he? Moreover, that the decline started before the mass vaccination program does not mean that the vaccination program had nothing to do with ending the outbreak. For example, by early December the government had expanded its state of emergency to ban nonessential travel:
Schools, shops, and businesses are shuttered. Children are forbidden from public spaces. And the entire population of 200,000 has been ordered to stay home and to hang out red fabrics if they want a mobile vaccination team to call.
Might this have had an effect before the vaccination campaign could truly take hold? I consider it likely. Marks also makes evidence-free claims that doctors were widely reporting that the disease they saw looked different than measles should. Given the lack of experience most physicians have with measles these days, thanks to mass vaccination and its near-elimination, I take these claims with a heaping grain of salt.
I will admit that I did laugh out loud—derisively, of course, when I read Marks’ assessment:
The current criticism of Kennedy is an endeavor to make him look dangerously ignorant and irresponsible to sway members of the Senate. Much to the chagrin of those who vilify him, his efforts to understand and assist in the Samoan measles outbreak exemplify his thoughtfulness and capabilities.
“Thoughtfulness” is not a word that I would ever associate with RFK Jr.
Conclusion
I’ve been writing about RFK Jr. for just under two decades now, starting with when he first “outed” himself as an antivaxxer, thanks to the co-publication of his misinformation-packed conspiracy-fest of an article, Deadly Immunity, which posited what I like to call the Simpsonwood conspiracy theory. This particular conspiracy theory is, of course, a subset of what I like to call the Central Conspiracy Theory of the Antivaccine Movement, namely that vaccines cause autism, harm, and death (and don’t work), but “They” (e.g., the CDC, FDA, state health departments, big pharma, the medical profession, and provaccine advocates) “cover up” the harm, all in the name of profit, ideology, and…well, I’m not sure what else, other than—if you listen to them—an apparent evil glee in harming and killing children. While I entirely expected the usual suspects (like the Brownstone Institute) to gaslight the public about one of the most vile things that RFK Jr. has ever done, contributing to the fear and uncertainty about MMR in the midst of an epidemic that was killing dozens of children on an island with a population of only around 200,000, I must admit that even I didn’t think that Dr. Prasad would “go there” and conclude something like this:
Ultimately, I find the narrative that RFK Jr is responsible for the measles deaths in Samoa to be a stretch. The time course doesn’t fit, and the root causes are systemic and multi-factoral, as is often the case in life.
It is not surprising that a poor island nation with poor health literacy, who 3 generations before never had the disease at all, would be highly skeptical of a medical intervention brought to them by those who previous brought the disease.
I think the MMR vaccine is safe and effective. But the US overall vaccine schedule is likely excessive (compared to Europe) and we need cluster RCTs and better safety systems.
Once again, just because the origins of the distrust of the MMR vaccine in Samoa that led to plunging MMR uptake rates that made the nation susceptible to a measles epidemic were due largely to the deaths of two babies because of an tragic and negligent error made by two nurses does not absolve RFK Jr. of his role in encouraging that distrust of vaccination in collaboration with local antivax activists like Edwin Tamasese and Taylor Winterstein. Nor does it absolve RFK Jr. of using his celebrity to write a letter to the Samoan Prime Minister (and the health minister) in which he tried to blame the epidemic not on low MMR uptake but on the MMR vaccine itself. That he did these things is a well documented fact that Dr. Prasad either knew but failed to mention or didn’t bother to find out. (I don’t know which would be worse.) Also note how he couldn’t resist signaling to his antivax audience that he thinks the US vaccine schedule is “excessive” and to repeat his call for “cluster RCTs.”
Tell you what, Dr. Prasad. Why don’t you write a few detailed posts that tell us exactly how, in your learned opinion, the US vaccine program is “excessive”? Which vaccines do you consider necessary? Which ones are “excessive” or unnecessary and should be removed from the schedule? (Show your work and cite the peer-reviewed scientific literature.) How, precisely, are our safety monitoring systems inadequate? (It would help if you actually understood, besides just the passive monitoring system VAERS, the active safety monitoring systems that exist, but you’ve seldom shown any indication that you have clue one about them.) More importantly, give us the details of exactly how we might conduct these “cluster RCTs” in an ethical fashion, complete with statistical justification to provide a minimum sample size that would provide the basis for an estimate of just how much conducting such a study would cost. (Hint: a lot.) Dr. Prasad won’t do it, because his statement that children are getting too many vaccines and his proposal for “cluster RCTs” are deeply unserious, meant to sound profound to his antivaccine readers without providing any actual scientific meat. I suppose he could prove me wrong, and I would admit it if he ever were to prove me wrong by actually writing detailed posts or articles enumerating exactly how the US childhood vaccine is “excessive” and how to do his proposed “cluster RCTs” of the childhood vaccine schedule, but I suspect that I am very likely safe from ever having to do that, as he never will.
But, hey, once again, I could be wrong. I just doubt that I am wrong. I also note that one big difference between Dr. Prasad and myself is that, whenever I write something, I always entertain the possibility that I might be mistaken, either about my overall narrative or about individual arguments and facts marshaled to support that narrative, and forced to rethink what I wrote when someone whom I’m criticizing shows me why I am mistaken using evidence and science. That is something that Dr. Prasad is always welcome to do, but somehow never seems to. I suspect that the possibility that he is in error is something that only very rarely, if ever, passes through Dr. Prasad’s planet-sized brain, which clearly views me as too trifling an annoyance to bother with. So the gaslighting will likely continue, both by him and RFK Jr.’s many other apologists.